A nursing report sheet is used by nurses in health establishments to obtain crucial patient information, which is then given to the nurse taking over the next shift.
This sheet is also known as a patient report sheet, an end-of-shift report, or a nursing brain sheet. It is vital for helping nurses monitor their patients when their shifts change. When nurses arrive for their shifts, they are given a report sheet from the nurses finishing their shifts. Thus, the report sheet is a concise and organized document for conveying important patient information used by the nursing staff.
A report sheet is necessary because it allows for a shorter period of transition between shifts by making the transfer of patients’ information between nurses quick and easy. In cases where patients are to be transferred to other units in the hospital, the report sheets are also handed over to the staff of the new unit.
Nurses, being the link between doctors and patients, are an important part of the healthcare sector, as are these report sheets. The reports contain vital information about patients’ diagnoses, allergies, attending doctors, treatments that need to be performed, medication times, vital signs, laboratory results, etc.
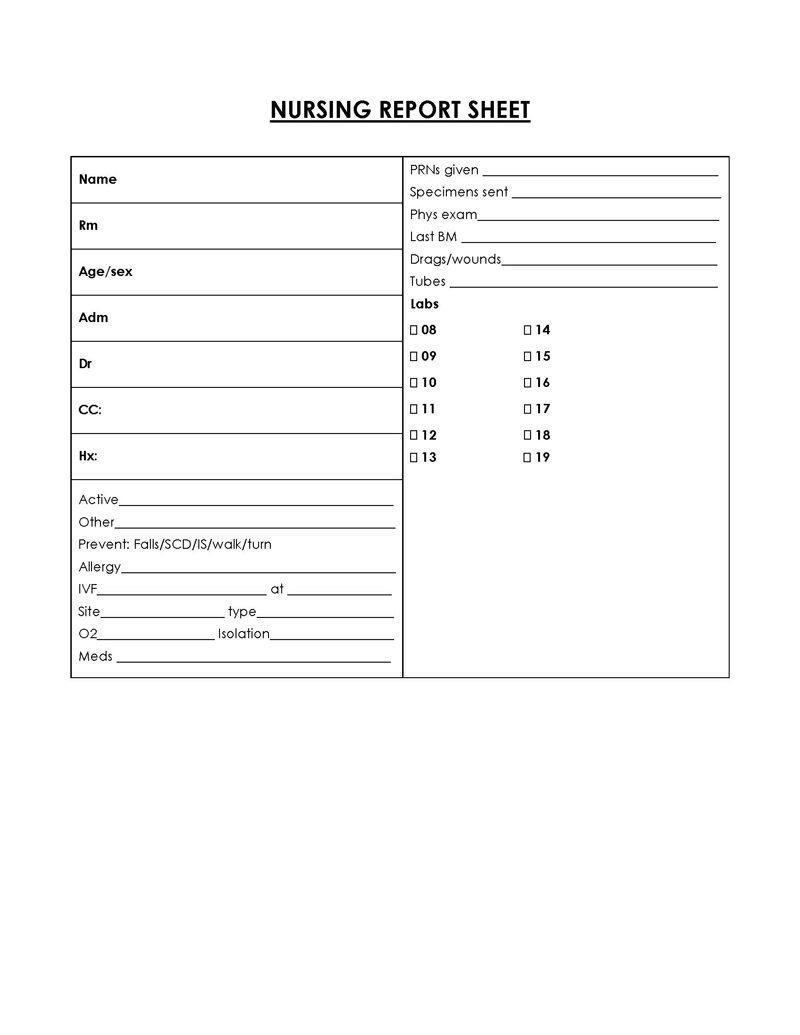
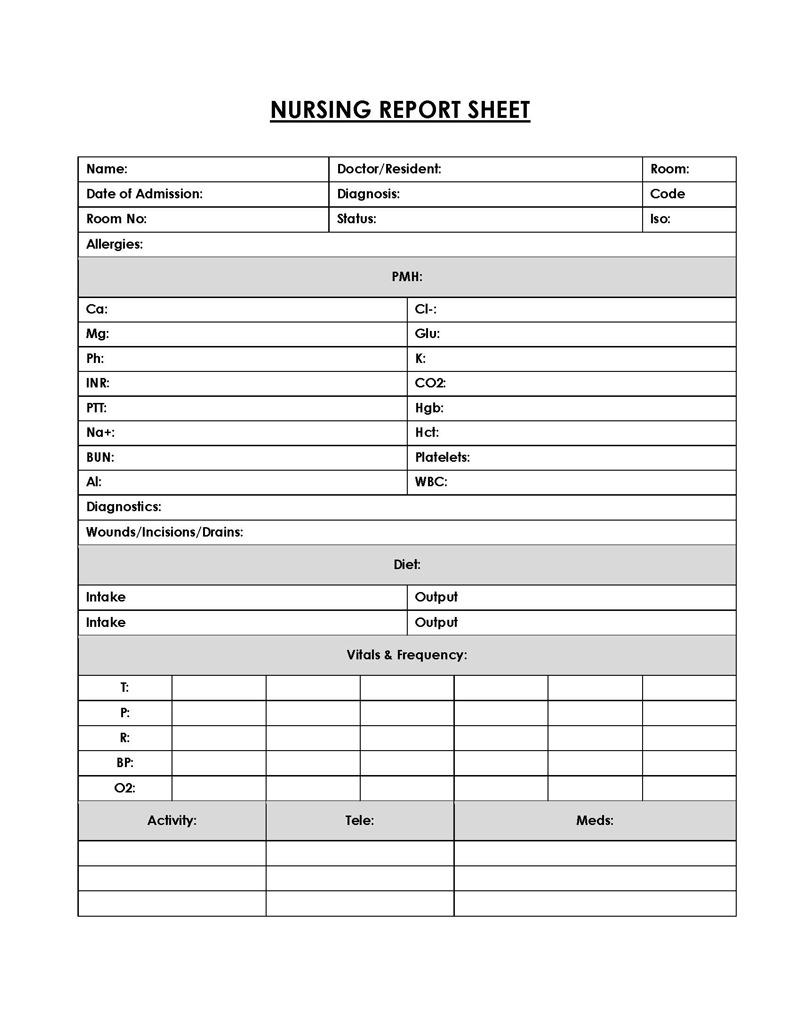
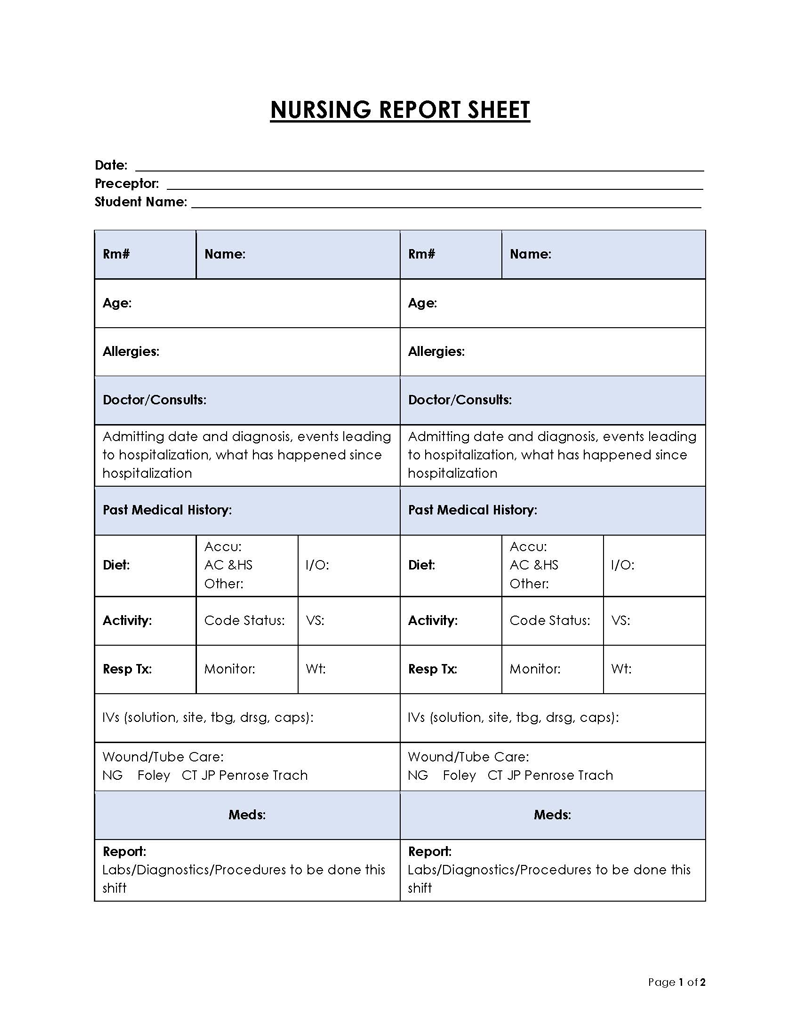
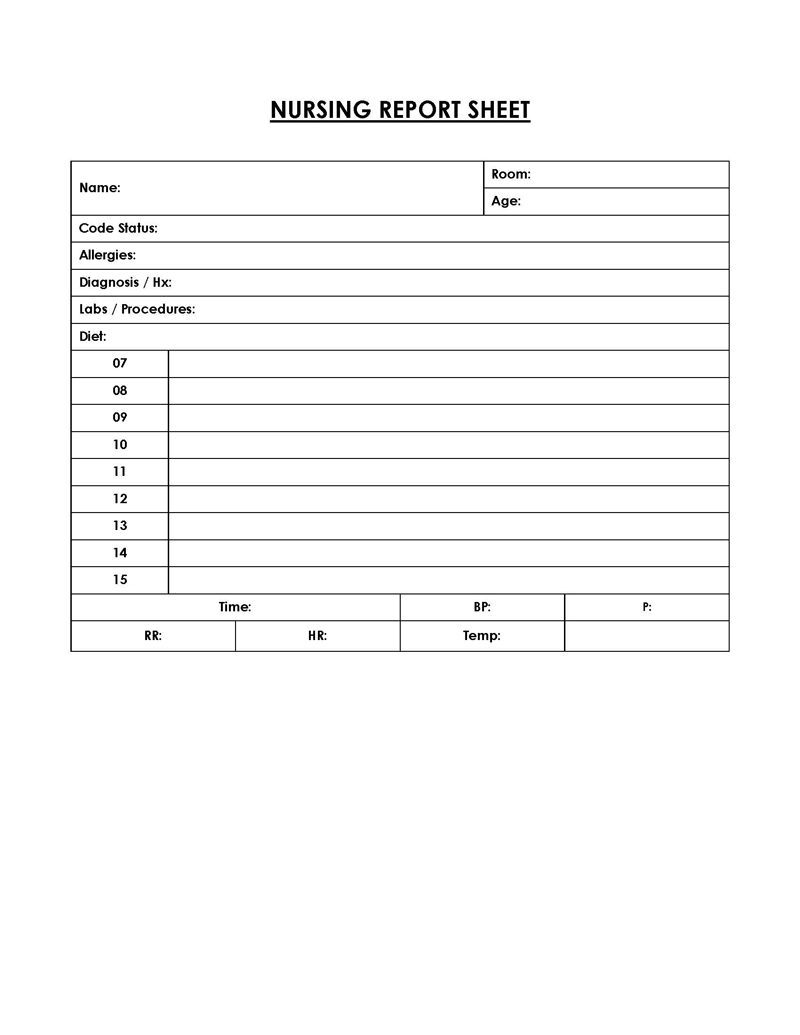
Free Templates
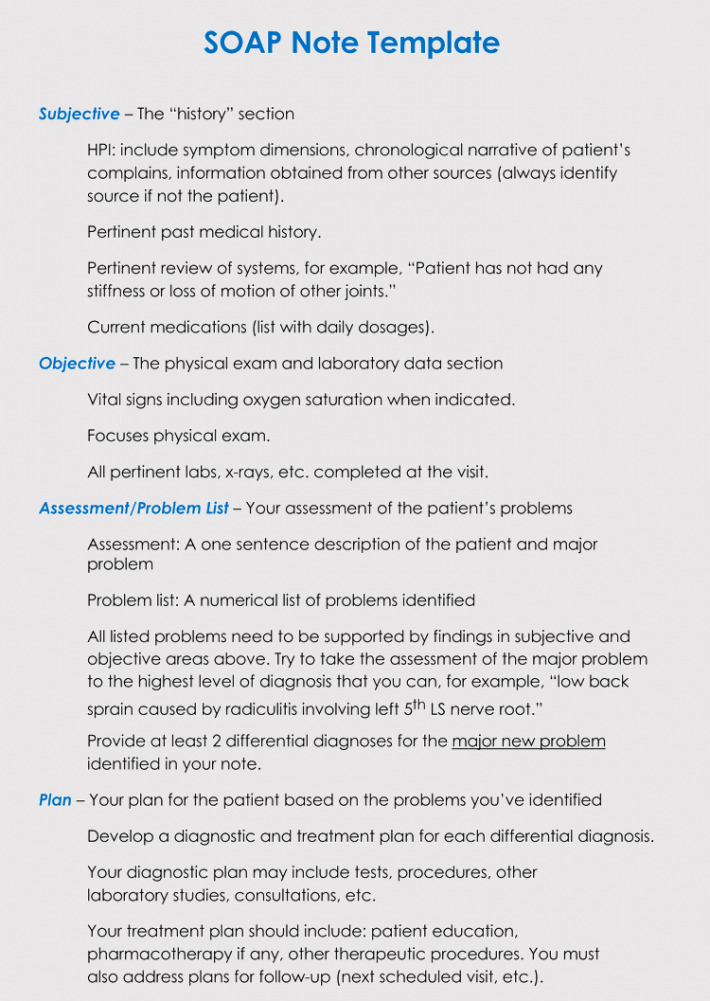
Nursing Report Sheet Vs. SBAR Tool
SBAR tool is an acronym for a situation, background assessment, and recommendation tool used as a guide for writing a nursing report. If you are unfamiliar with the differences between an SBAR tool and a nursing report sheet, it may be challenging to distinguish between them.
An SBAR tool contains patient data that might not be included in the sheet, such as the patient’s medical history, the current state of health, necessary actions, and more.
Although they are not the same thing and contain different content, nurses can use an SBAR tool and the report sheet simultaneously. This is because the information about a patient in an SBAR tool is often a great help in completing the report sheets.
Furthermore, an SBAR tool also helps to provide a framework for communication between members of the healthcare team about patients’ conditions.
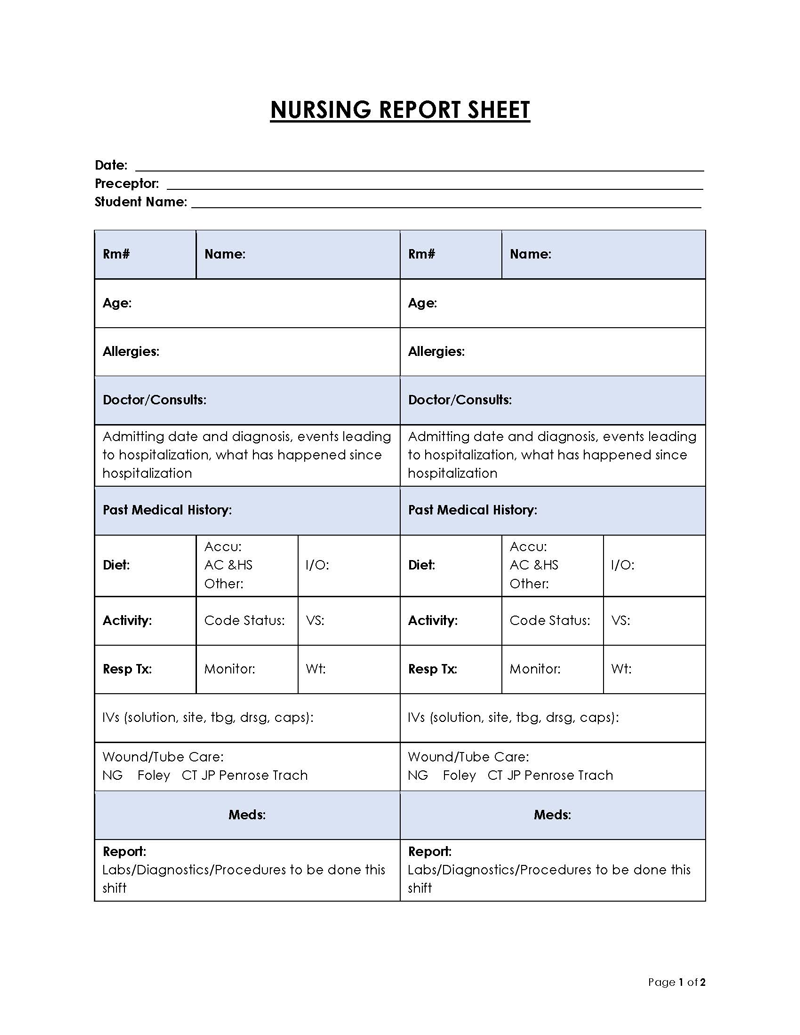
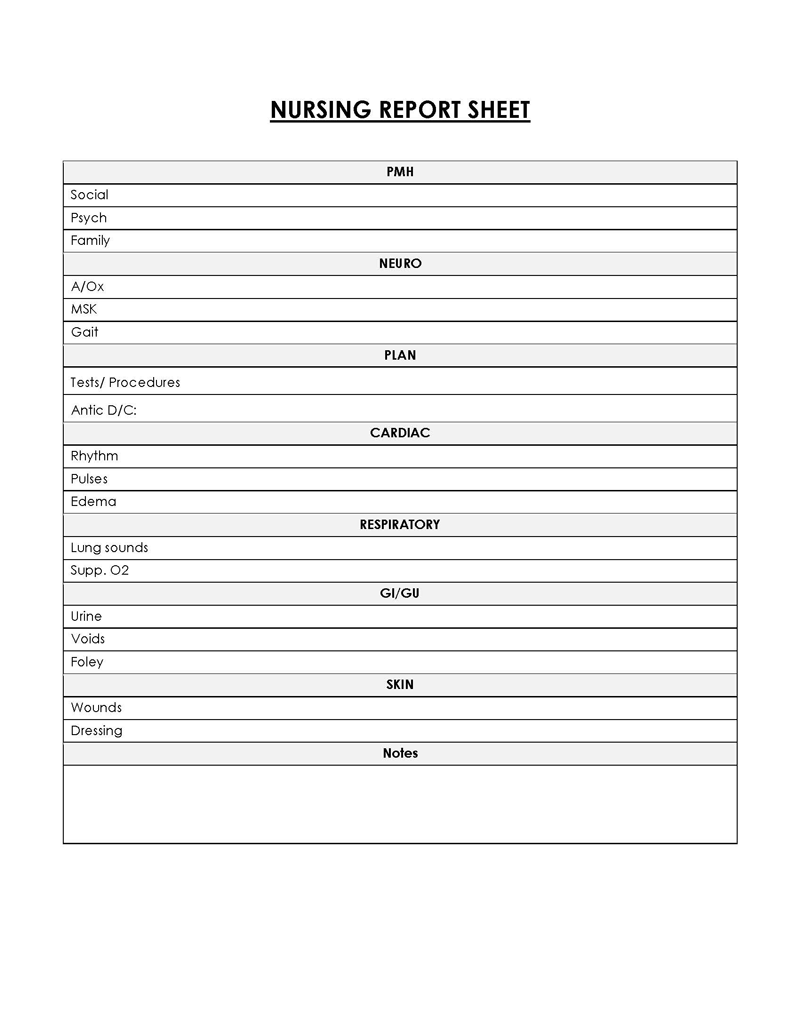
What to Cover in a Nursing Report Sheet?
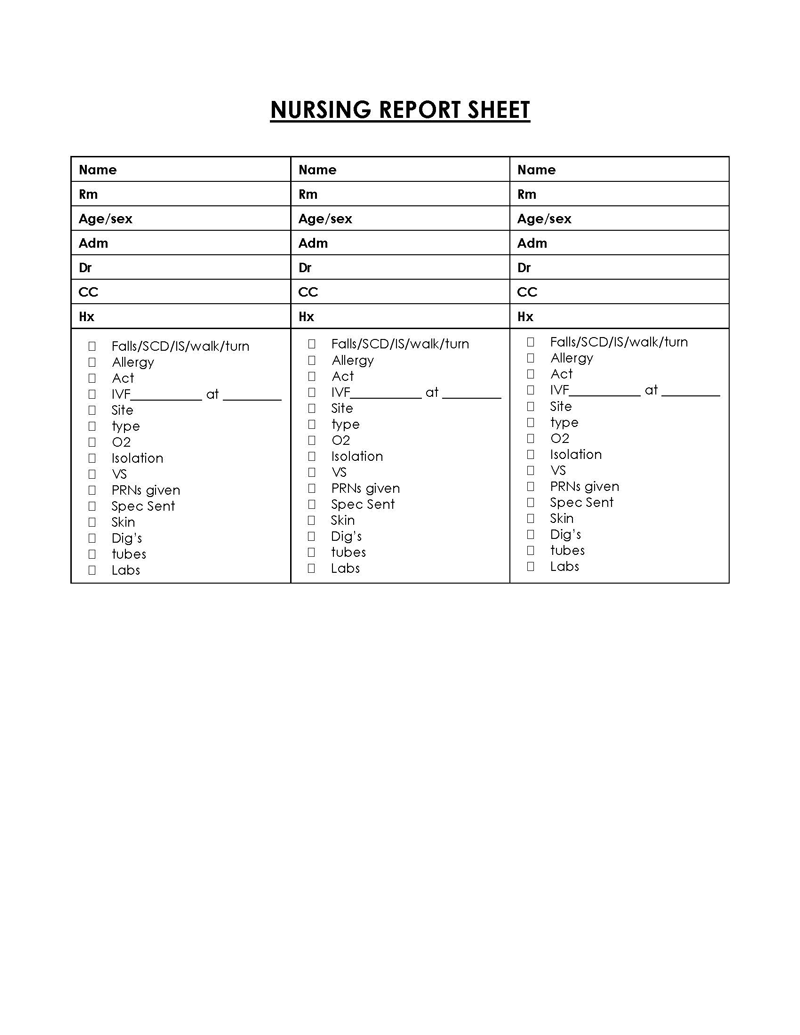
When creating the sheet, there are important categories that must be included. This is done to make sure that the nurses arriving for the next shifts receive accurate patient information that has been recorded.
These categories include:
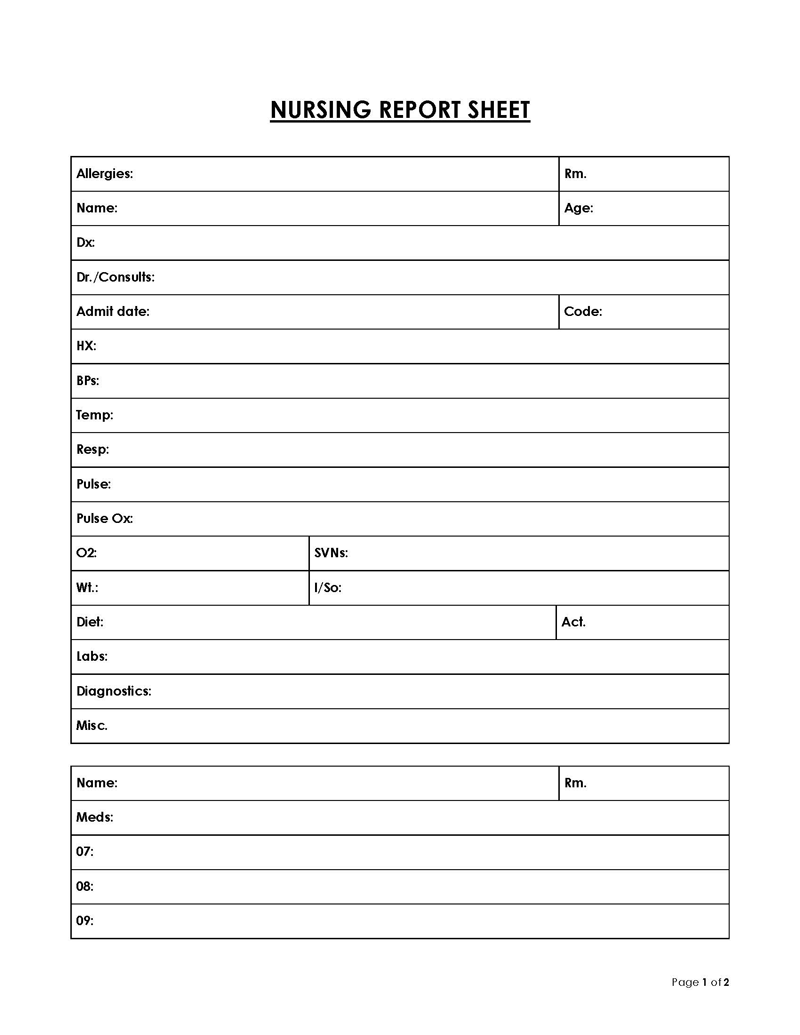
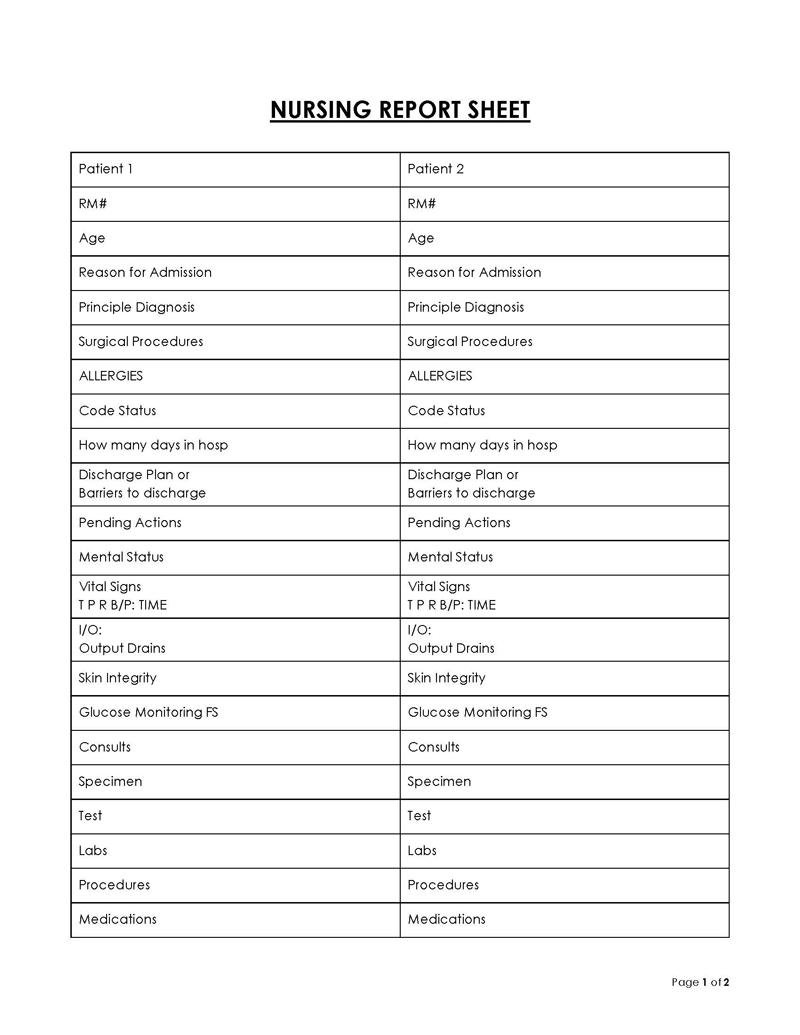
Patient’s basic details
This is the primary information that should be recorded in the sheet. The basic details of patients, such as name, age, and code status, that point to the identity of the patients, should be mentioned. By doing this, any treatment-related misunderstandings that might arise due to the report sheets’ failure to include patients’ names are avoided. The code status reflects the patients’ identical relevant medical conditions. You should also note any possible allergies the patient might be prone to.
Other basic information that may be useful is the patient’s room number, date of birth, details of their power of attorney (next of kin), the date of their admission into the hospital, the name of the doctors treating the patient, any advanced directives, an updated record of their diagnosis, and details of their medical history, amongst other things.
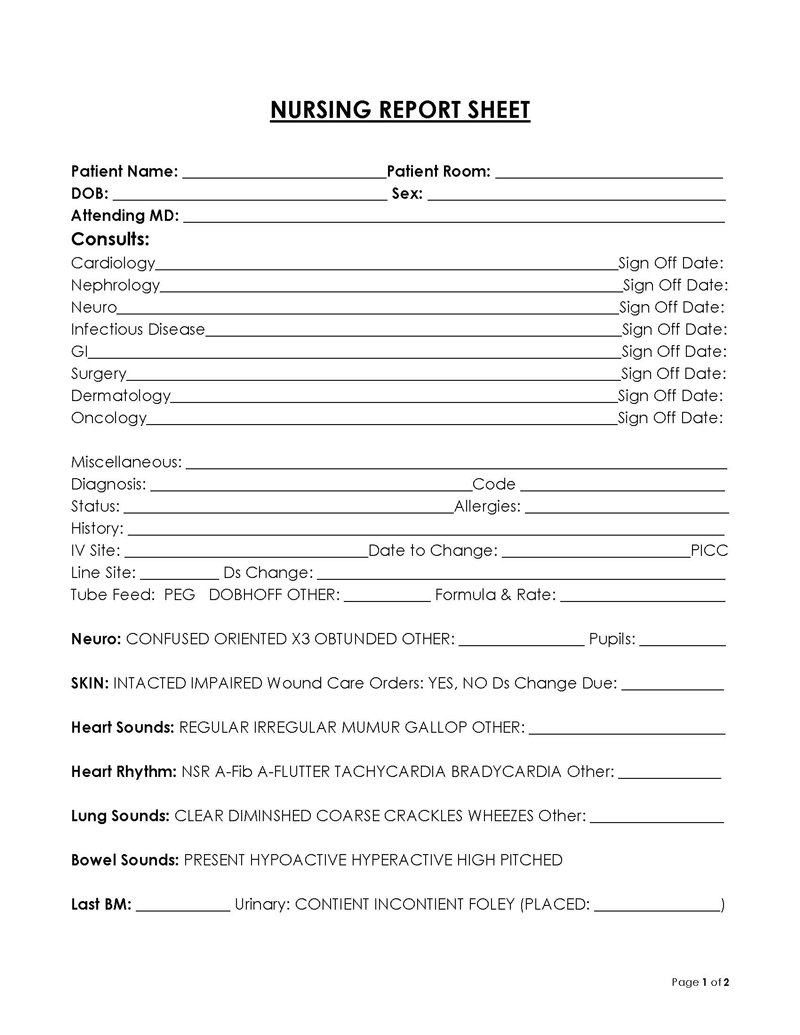
Information about the attending doctor
The name and other information of the doctors attending to patients should be mentioned on the report sheets. Indicating the names of medical doctors or physicians helps to know the right personnel to be updated about the patients. So, make sure to enter information about the medical doctor or physician assistant treating patients in the appropriately indicated sections on the report sheet. For example, the medical doctor’s details should be in the MD section, while the name of a nurse or physician assistant should be in the NP/PA section.
Medical history of the patient
The medical history of patients should be mentioned in the spaces made available for it on the report sheet. It should contain recent medical conditions or those associated with the health issues affecting the patients at that given point. Ensure that you only include relevant medical conditions or past incidents because there is limited space available on the form.
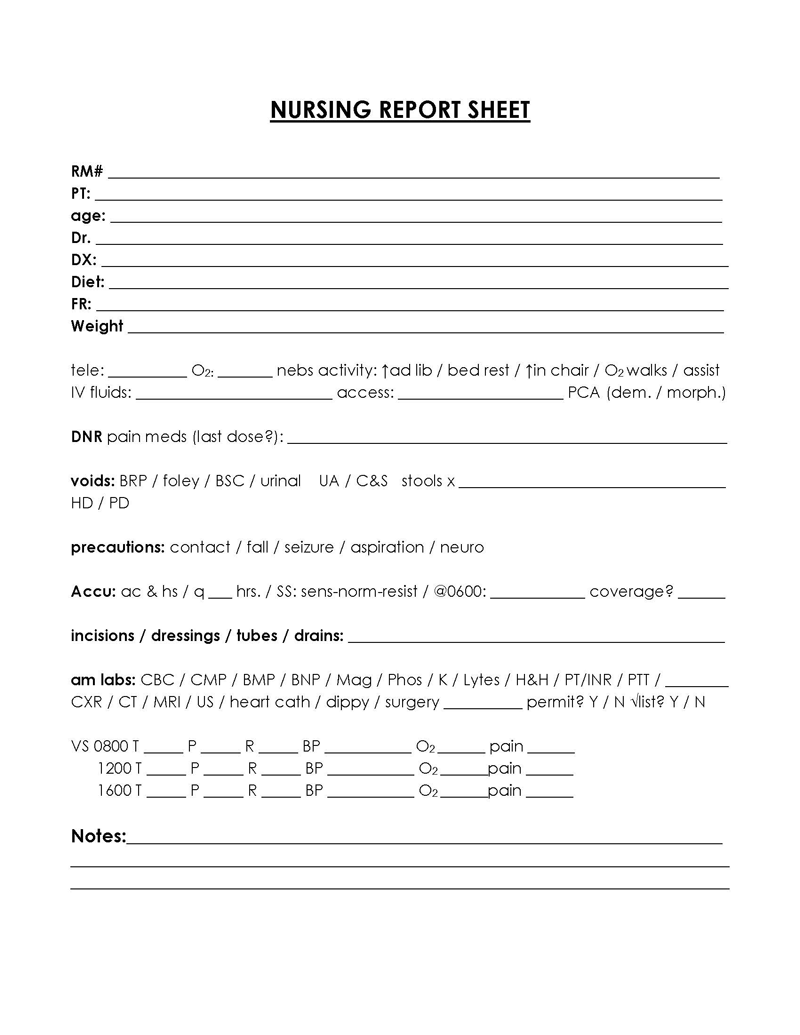
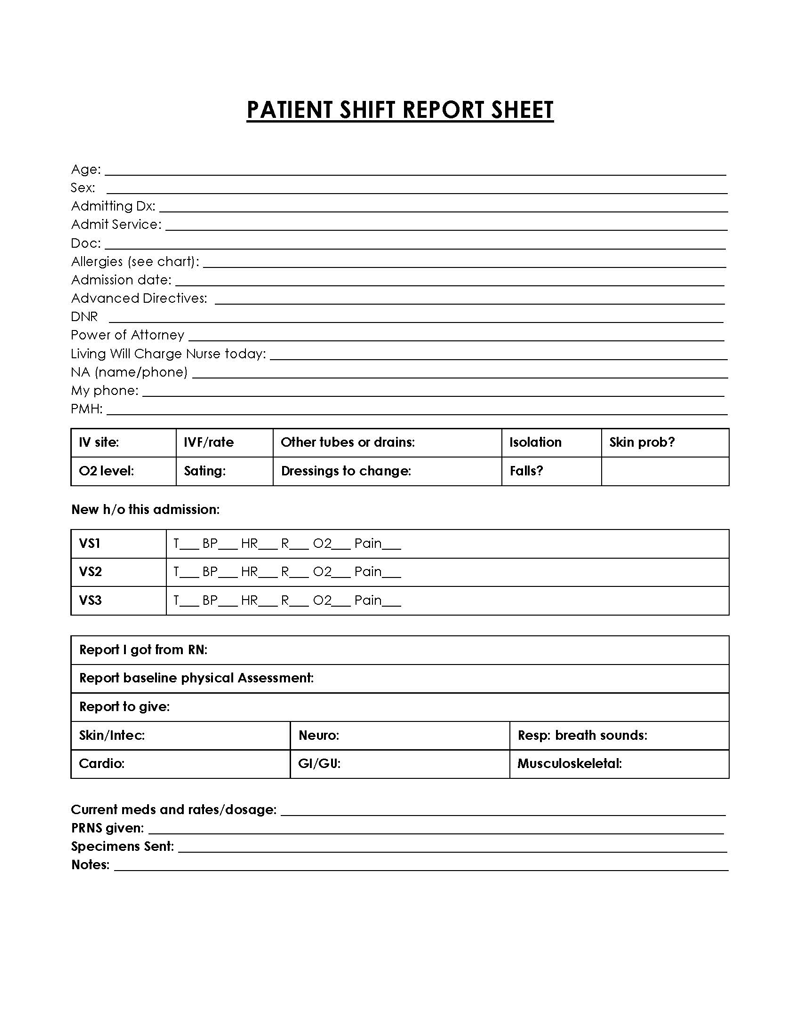
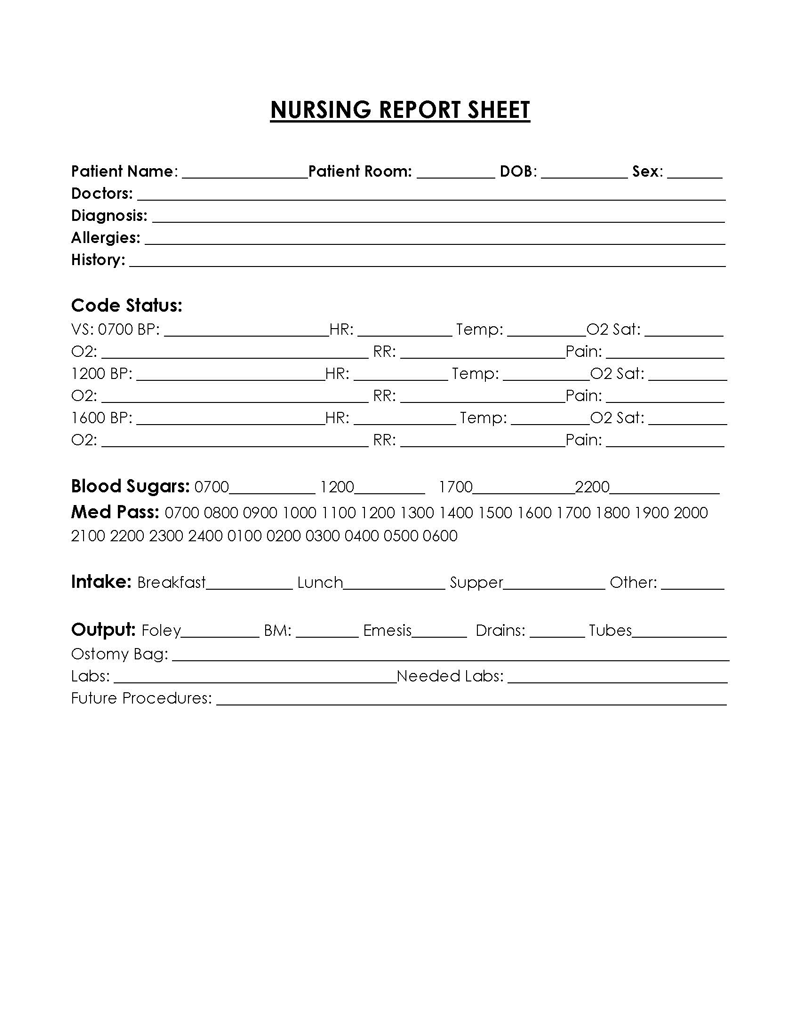
Patient’s current health information
Apart from a patient’s relevant medical history, a reporting sheet must contain the patient’s current health information, because it determines the patient’s state of health and the medical treatment to be administered. It includes neuro information, which reveals the level of consciousness of the patient; the patient’s dietary restrictions or urinary considerations (if they need catheters), the condition of their skin, and if there are any wounds present that require care, as well as the type of IV fluid the patient is receiving.
These vitals should be mentioned in the correct spaces on the sheet indicated as Neuro (neurological activity), CVS (cardiovascular system), Skin, and RESP (information about their respiratory systems), among others.
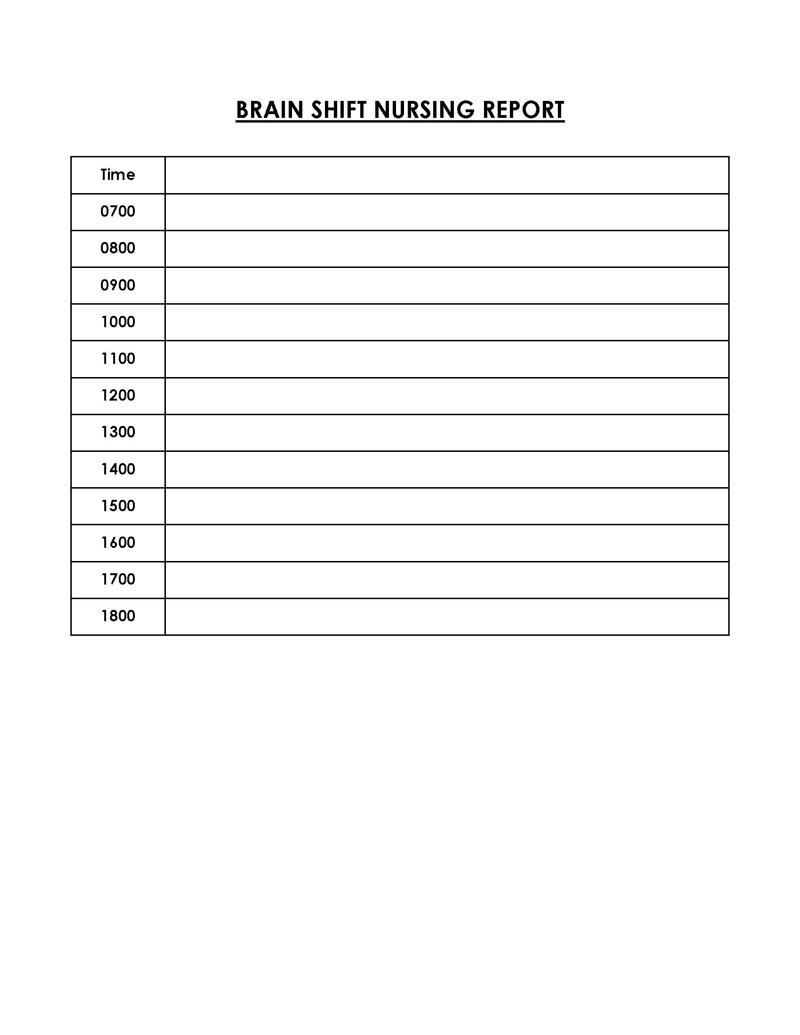
Ongoing patient care
If they are regularly monitored, the report sheet must list every medication and ongoing care that was given. The ongoing patient care information mentioned on a report sheet should mention the dosages of medications being administered, the dates to undergo certain tests, their readiness for discharge, or their estimated duration of stay.
Future procedures
If patients have any upcoming procedures, this information is vital to include in the report sheet. The nurses taking over the next shift must be aware if patients have any upcoming procedures that they should be prepared for in advance.
Patient notes and recommendations
The notes and recommendations are used to explain things that are not included in the sheet. For instance, it must be mentioned that a translator might be needed if the patient speaks a different language. The notes and recommendations may also contain things like the patient’s routines, noteworthy triggers, special dietary requirements, room temperature, etc.
What Should be Excluded?
Although the report sheets are meant to contain vital information about patients, that does not mean that they must contain every single personal and medical detail. There are some sections where details are not needed because they are not relevant to the existing health condition or they can easily be accessed by the nurses. Remember that it is common for nurses to make several reports at the same time, so reducing the amount of time spent on a single patient’s report is necessary.
Below are some of the things that should not be included in the report sheets:
Patient’s non-essential comorbidities
While it is advised to mention patients’ medical conditions in report sheets, only the primary ones and not the non-essential comorbidities that the patient may be experiencing should be included. This is because the patients may have multiple comorbidities, and mentioning them would require extra time and use extra space on the sheet.
Every medication the patient takes
Following the same principle of mentioning only vital and important information, the sheet should only include important medications that are specific to patients. This is because patients are usually using multiple medications, and the nurse on the next shift can easily check them. So, it is advisable to only mention medications that are specific to the current diagnosis.
Patient’s laboratory test results
This information is also not necessary to be included in a report sheet. Patients’ specific laboratory test results can be acquired by any nurse if needed because the information is usually readily accessible in a hospital.
Benefits of a Nursing Report Sheet
Having learned about what the sheet is, it is also necessary to outline why it is important for nurses. Outlined below are some of their benefits:
- It provides necessary information about patient care to the nurses taking over shifts who may be unfamiliar with the patients and their medical needs.
- It allows nurses to have fast and easy access to vital patient information so that when doctors ask you about a particular patient’s condition, it can be easily accessed to find key information required by the doctors.
- If nurses have to deal with multiple patients during their shifts, then report sheets on each patient will help to differentiate the patients and not mix up their treatments and medications.
- A report sheet also serves as a reminder that helps to monitor the medications and treatments needed before the end of shifts.
- Another benefit is that it helps with charting accuracy. It increases the ease and accuracy of charting because it would be more accurate and easier to do when written on a report sheet or multiple reports if more than one patient is being tended to.
- Since creating a report sheet may serve as a reminder for nursing activities, it ultimately results in better time management because it helps specify shift duties.
- It can also serve as a legal document showing the type of medical care a patient receives in a medical establishment if there is a need. Also, a nurse’s proof of due diligence can be confirmed through the entries on the report sheet.
- Nurses who diligently adhere to the routine of report sheets can actively improve the safety and care of patients. This is because even when off duty, the incoming nurses would already have ideas on how to adequately care for patients whose details have painstakingly been monitored.
Conclusion
The importance of nurses in healthcare cannot be overemphasized. Nurses play a major role in managing the healthcare system by ensuring continuity and accountability while working with doctors to take care of patients. This is achieved by maintaining a nursing report sheet where vital patient details are recorded and shared when necessary.
This article has provided a general overview of what a nurse report sheet is, why it is important, and what must be included in it. It has also provided free templates for use. Following the guidelines given in this article, you should be able to customize a professional and detailed nursing report sheet that would help you and your colleagues perform your nursing duties effectively.
About This Article